Addressing Ethical Challenges in Healthcare
[easy_youtube_gallery id=YTuSF_2BLAg cols=1 ar=16_9 thumbnail=0 title=top]First Video[/easy_youtube_gallery]
Yogyakarta, February 26, 2025 – The Center for Bioethics and Medical Humanities (CBMH) Universitas Gadjah Mada once again held its regular webinar, Raboan Sharing & Perspective Sharing. This webinar was conducted online via Zoom Meeting and featured Dr. Bondan Agus Suryanto, S.E., M.A. (Lecturer at the Faculty of Medicine, UII and FMPHN UGM) as the main speaker, with Mahmasoni Masdar, S.Kep., Ns., M.Kep as the moderator.

Presentation by dr. Bondan Agus Suryanto, S.E., M.A.
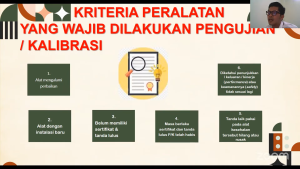
This session explored “Ethical Issues in Healthcare Services”, highlighting challenges and solutions in achieving fairness in the distribution of healthcare services. In his presentation, dr. Bondan emphasized the importance of a bioethical approach based on social justice to ensure equitable healthcare access amid limited resources. Additionally, he discussed the role of professional organizations in maintaining a balance between the interests of healthcare professionals and the needs of the broader community.

Interactive Discussion with Participants
Mahmasoni Masdar, as the moderator, led an interactive discussion involving participants from various backgrounds, including healthcare professionals, academics, and students. The session delved deeply into different perspectives on healthcare ethics in Indonesia, covering public policy roles, the influence of culture and religion, and challenges in implementing a health insurance-based system such as BPJS.
The discussion on ethical issues in healthcare services aligns with the Sustainable Development Goals (SDGs), particularly SDG 3: Good Health and Well-being and SDG 10: Reduced Inequalities. This webinar aimed to foster cross-sector dialogue to help design more equitable healthcare policies, ensuring that every individual, regardless of social and economic background, can access quality healthcare services.
CBMH UGM hopes this forum will serve as a platform for stakeholders to engage in discussions and share insights on bioethics in Indonesia. Through cross-sector collaboration, the goal is to develop healthcare policies that are fair and easily accessible to all.
Reporter : Alvira Rahmasari, S.H.G.
Editor : Rafi Khairuna Wibisono, S.Kom.